Are all arch development techniques created equal?
The debate between the fixed and removable or rapid and semi-rapid expansion camps has been raging for decades. Regardless of the type of arch development technique, the aim is more or less the same: turn a screw and expand the mid-palatal suture. Very few question this dogma, but is this the best approach to arch development?
For the published PDF version click here
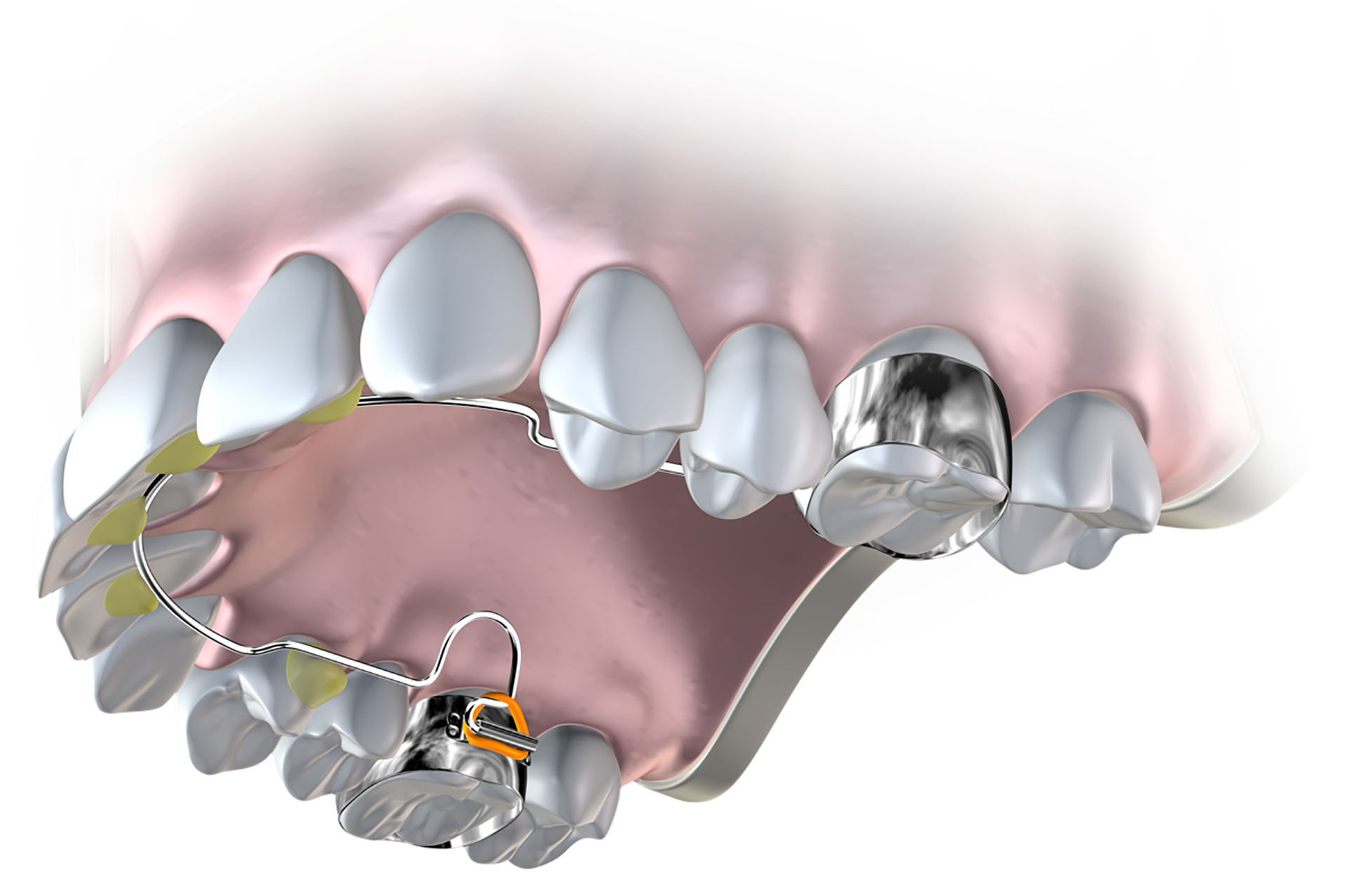
Figure 1. The Farrell Bent Wire System™ - a simple and effective expansion approach combined with The Myobrace® System.
Donald Enlow is widely considered as one of the greatest researchers in craniofacial growth. In fact, you would be hard pressed to find an orthodontic school who does not teach his concepts. Although many clinicians have read his highly influential book, Essentials of Facial Growth, few take notice of this paragraph:
"Historically, the process of expanding the maxilla by ‘splitting’ the mid-palatal suture has been thought of as a ‘biologic’ procedure. Such is not the case. The mid-palatal suture probably plays a small role, if any, in the displacement of the maxillary shelf laterally."[1]
According to Enlow, the techniques employed to separate the mid-palatal suture have no basis in the normal process of growth and development. Furthermore, such a traumatic procedure, although widely employed, has been previously reported to have serious side effects in some patients and may be affecting others in ways we haven’t anticipated.[2],[3] Many readers will be asking themselves, if splitting the mid-palatal suture is not the right way, then what is? Before we can answer this question, we must first understand how the arches develop.
RELATED: 'How myofunctional orthodontics relates to every dental practitioner' by Dr Emad Ahangari
The theories of Enlow, Moss and others, are commonly known in orthodontics.[4] These authors proposed that although the genes play a guiding role in facial growth, the function and growth of the soft tissues are the primary drivers. Nasal breathing in combination with the correct tongue to palate contact and correct function of the peri-oral muscles is crucial in driving the correct development of the upper jaw and dentition.[5]
From this knowledge, it follows that the re-establishment of correct breathing and oral muscle habits, from as early as possible in growing patients, is an essential endeavour if we are to give patients the best chance of developing correctly.
The issue that we face currently is that virtually all expansion appliances occupy space across the palate, which worsens the patient’s tongue position and will invariably affect swallowing patterns and breathing, particularly during sleep. These atypical habits that are caused or worsened by expansion techniques which occupy space across the palate will logically deteriorate patient function. Perhaps this may also explain poor stability in expansion cases.[6]

Figure 2. This 9-year-old female patient is still in treatment, but shows the power of the BWS and Myobrace® combination in creating arch development.
Since they work on the suture, almost all expansion appliances develop mainly in the transverse dimension. Although research has shown that this opens the nasal cavity and decreases resistance to airflow, a good portion of the change may be due to the sagittal development of the maxillary structures which occurs as a side effect of expansion and not only lateral development of the nasal cavity.
Forward displacement of the upper jaw results in increasing nasopharyngeal dimensions and perhaps more crucially, the translation of the lower jaw and tongue anteriorly, improving muscle tone around the velopharynx and base of the tongue, factors commonly implicated in sleep breathing disorders.[7]
If we are also to create more room for the tongue to move upwards and forwards out of the airway and rest against the palate, expansion should be performed in the transverse and sagittal dimensions together. As the structures are being developed, all efforts should be directed at simultaneously correcting the patient’s breathing and oral muscle habits so that optimum natural development is achieved in addition to the mechanical expansion.
Thinking of these issues as only structural, as opposed to a combination of structural and functional components, is highly flawed and unidimensional thinking. Since function and structure reciprocally affect one another, expansion and habit correction should be done together and not staggered one after the other. As a bonus, three-dimensional expansion invariably creates more space for the teeth, as opposed to expansion that only occurs in two dimensions.
We now understand the shortcomings of mainstream expansion techniques and how we should be thinking about approaching arch development. Unfortunately, for many decades, the profession lacked any solution which could develop the arches in three dimensions, avoid trauma to the mid-palatal suture, while simultaneously improving patient function.
The Farrell Bent Wire System™ (BWS) from Myofunctional Research Co. (MRC) was developed precisely to meet this demand. The BWS is a lightwire arch expansion technique, which develops the arches in three dimensions while avoiding any traumatisation to the mid-palatal suture and interference with patient function. It must be combined with specially designed Myobrace® appliances which simultaneously improve patient function, while the BWS develops the arches.
DOWNLOAD: Our FREE Arch Form & Orofacial Muscles Infographic
In addition to these biological benefits, there are practical benefits too. The BWS can be made in-house by trained auxiliaries in less than 10 minutes, while costing a few dollars per appliance. It doesn’t interfere with patient speech and is invisible to outside viewers, which makes it well accepted by patients. The BWS is adjusted every four weeks, harnessing the superiority of intermittent forces over continuous ones, while the adjustment appointment itself is extremely simple, taking less than two minutes to complete.
The power of the BWS is illustrated in Figure 2. This nine-year-old female patient attended MRC’s clinics with the complaint of severe crowding and mouth breathing. In combination with the Myobrace®T1BWS, the BWS appliance was used, demonstrating the impressive expansion achieved. The patient’s function is completely resolved and she is habitually nasal breathing while awake and asleep.
This case is still in treatment and used for illustrative purposes, yet it shows that the BWS and Myobrace® combination can correct some of the more severe cases of arch restriction. Practitioners who would like to learn about the aforementioned techniques can do so by visiting the Online Courses section of this website. Recently, the release of the Farrell Bent Wire System™ course allows practitioners to gain an end to end understanding of the BWS, including how to fabricate, fit and adjust the appliance.
Interested in learning the BWS arch development technique?
Our Farrell Bent Wire System (BWS) course provides an overview of the arch development technique most commonly used during Myobrace treatment and covers key components required to fabricate, fit and adjust the BWS effectively.