A resolution to the limitations of orthodontics
For the published PDF version click here
Traditionally, orthodontics has focused on the treatment of teeth alone, instead of the patient as a whole, including its effect on the facial profile and muscle function. We now understand there is an aetiology to malocclusion.[1][2]
Therefore, practitioners should consider treatment options that not only provide an aesthetic result, but also address the underlying causes.
This was highlighted in a recent case report titled Treatment of Class II Div I malocclusion with the combination of myofunctional trainer and fixed appliances from the October 2019 edition of the American Journal of Orthodontics and Dentofacial Orthopedics.
RELATED: 'The 6 Rs of Orthodontics: Part 1 – Relapse' by Dr Chris Farrell
The report demonstrated the importance of both structural and myofunctional approaches in order to optimise treatment results.
Furthermore, the review found the combined approach to treatment achieved muscular functional exercises, expanded the maxilla transversely and stimulated growth of the mandible, providing optimum patient comfort with minimum appliance thickness.[3]
However, practitioners should also ponder if there are additional indicators for treatment optimisation. Research indicates that early intervention is the ideal treatment to enable the correction of myofunctional problems and develop the jaws.[4][5][6]
The Myobrace® for Braces series can be used to correct muscle dysfunction in conjunction with traditional orthodontics.
Nevertheless, there is still merit in correcting the muscle dysfunction with older patients[4] to allow better stability of the results along with quicker progress.
The power of incorrect muscle pressure on bone and jaws has been recognised for more than 50 years, yet it is only recently that there has been more emphasis on soft tissue dysfunction and establishing correct nasal breathing in diagnosis and treatment planning.
Muscle dysfunction can hinder treatment progress,[8][9][10] consequently prolonging braces treatment time and the persistence of the dysfunction after treatment can contribute to relapse.[11][12]
Therefore, by supporting orthodontic movement with myofunctional therapy, the result will be less aberrant muscle pressure on the teeth, allowing the brackets and wires to move more freely, enabling the practitioner to develop the arches better, quicker and produce a more stable end result.[2][5]
CASE STUDY A: FEMALE, 18 YEARS OLD
The patient’s main concern was her crooked teeth, narrow jaws and anterior open bite. The patient wanted a more holistic approach to treatment and to not have prolonged braces treatment due to her age. Patient A was treated with upper braces along with the Myobrace®B1 for initial upper expansion and function retraining. Lower braces were then fitted once expansion and function had improved.
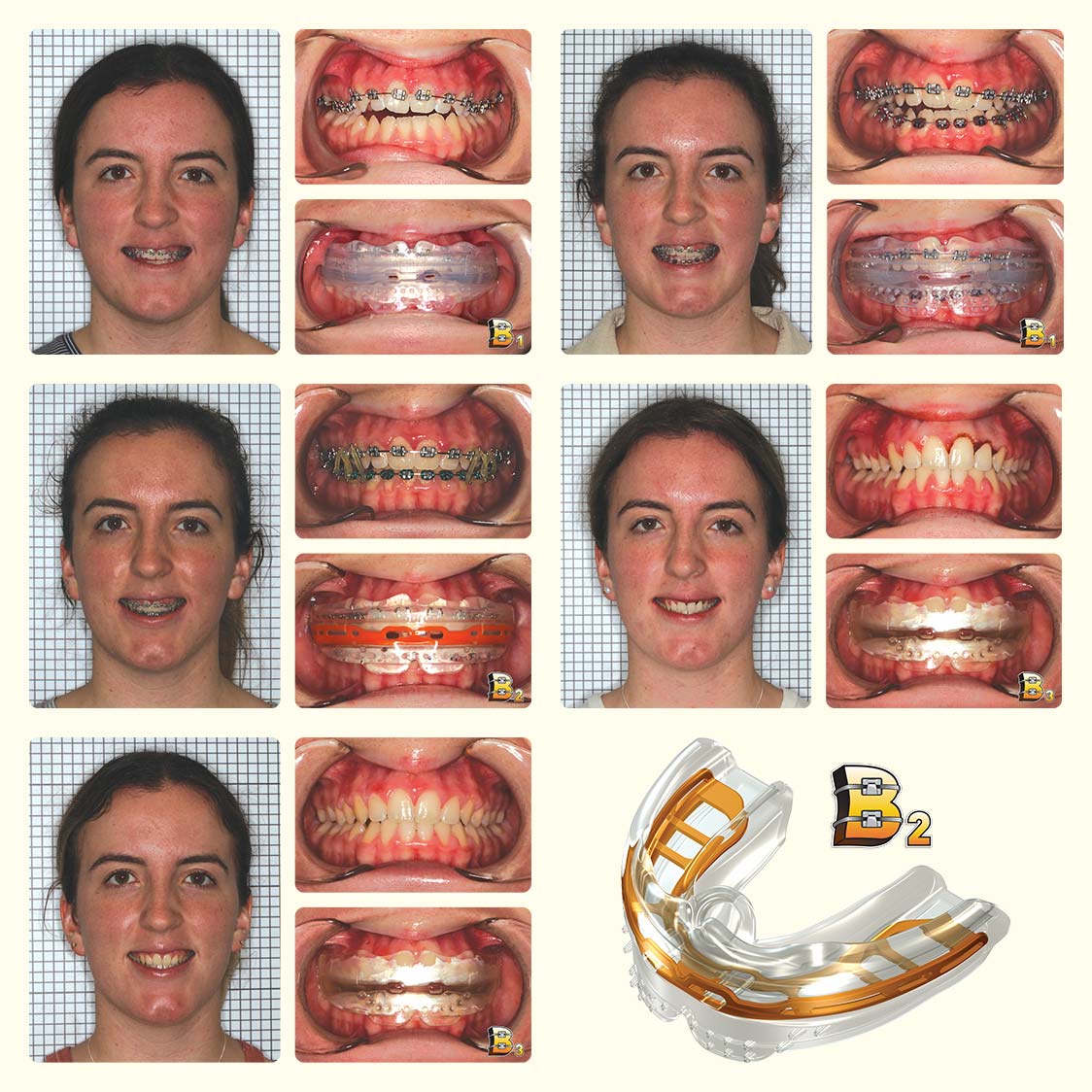
Top row: Start of treatment - upper braces fitted + Myobrace® B1 & Four months into treatment - lower braces fitted + Myobrace® B1; Middle row: Nine months into treatment - inter-arch elastics + Myobrace® B2 & 14 months into treatment - deband, gingivectomy for #21 and #22, removable thermoformed retainers and Myobrace® B3 issued.; Third row: Retention recall four months post-treatment & Myobrace® B2.
Once lower alignment improved, the patient progressed to the next stage in wires and appliances with the Myobrace®B2 in combination with inter-arch elastics. Alignment and occlusion were finalised by 12 months of treatment, braces were removed at 14 months with removable thermoformed retainers and the Myobrace®B3 was issued for post-treatment retention.
Once correct diagnosis is established, the ideal orthodontic treatment should initially address any functional concerns - focusing on airway, tongue posture and range, correct swallowing pattern and correct lip seal.
Orthopaedic concerns should be addressed at the appropriate time for growth[13][14] and lastly, dental concerns should be addressed through orthodontics.
TREATMENT: Learn more about the Myobrace®B-series
The Myobrace®System offers a range of appliances which can be used in conjunction with fixed braces treatment to provide the patient with a better overall result by improving alignment, jaw position and function simultaneously.
It is important to consider long-term retention when treatment planning for longevity of results. Keys of retention should be correction of soft tissue (i.e. frenums, tongue ties, etc), correct hard tissues (i.e. parallel roots, good intercuspation, etc) and correct function (establish nasal breathing, lips comfortably together at rest, correct tongue resting posture and correct swallowing pattern).
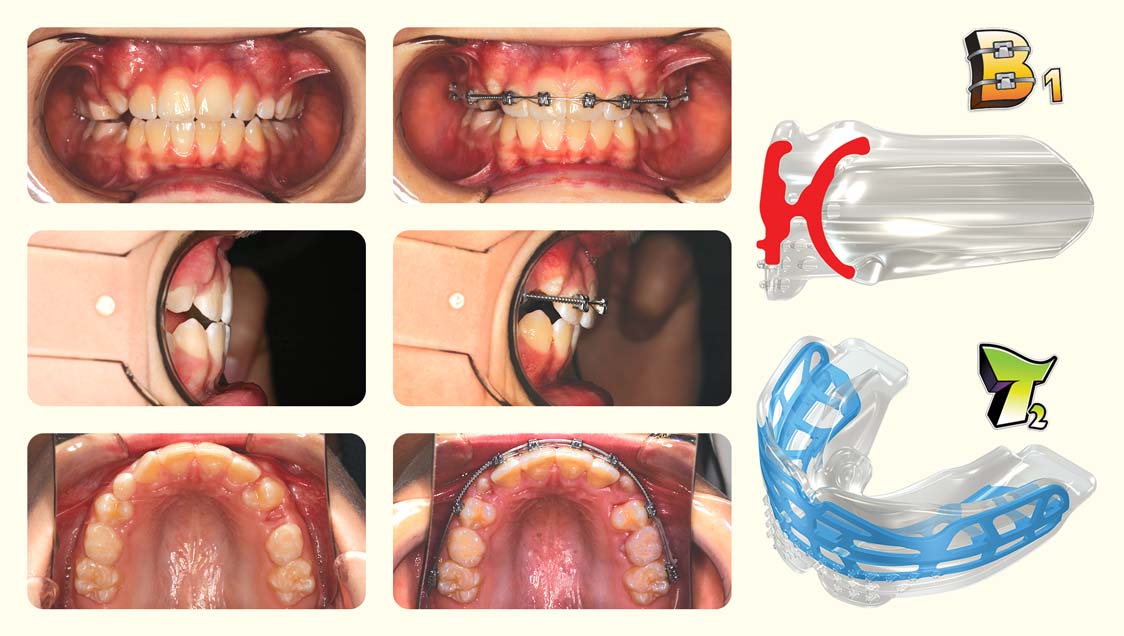
CASE STUDY B: FEMALE, 12 YEARS OLD
The patient’s main concern was to improve the alignment and occlusion; however, the parents did not want any extractions or interproximal reduction (IPR). Patient B was treated with upper braces along with the Myobrace®B1. The patient then progressed to the Myobrace®B2, as there was not enough positive overjet to fit the lower braces without performing any IPR.

Top row: Start of treatment; Second row: Three months into treatment; Third row: Seven months into treatment; Bottom row: Completion of treatment after 15 months.
Once sufficient positive overjet was created, the lower braces were fitted and the patient went back into the B1 initially, then back to the B2 once more comfortable. Patient B finished treatment with a positive overbite and overjet, in 15 months of treatment, and was issued a removable thermoformed retainer and the Myobrace®B3.
Orthodontic treatment can be particularly challenging in patients with severe muscle dysfunction. Therefore, by including a functional appliance in conjunction with the orthodontic treatment, challenging cases can be converted into more easily treated cases.[12] Regular fixed appliances (brackets, bands) are not considered disturbances to the myofunctional therapy.[15]
The first two case studies in this article demonstrate anterior open bite patients who have low tongue posture and incorrect swallowing pattern with associated tongue thrust. These otherwise difficult cases[7] were managed simply and quickly by combining braces with the Myobrace®for Braces range.
CASE STUDY C: MALE, 11 YEARS OLD
The patient presented with the upper left premolar erupted in the upper left canine position.
Left column: Start of treatment.; Middle column: Three months into treatment; Right column: Myobrace® B1 and T2.
Patient C was treated with upper D-gainer braces therapy for 10 months to move the premolar distally and make room for the canine teeth, in conjunction with the Myobrace®B1 to maintain the correct occlusion and allow the lower jaw to adapt with the new upper arch shape.
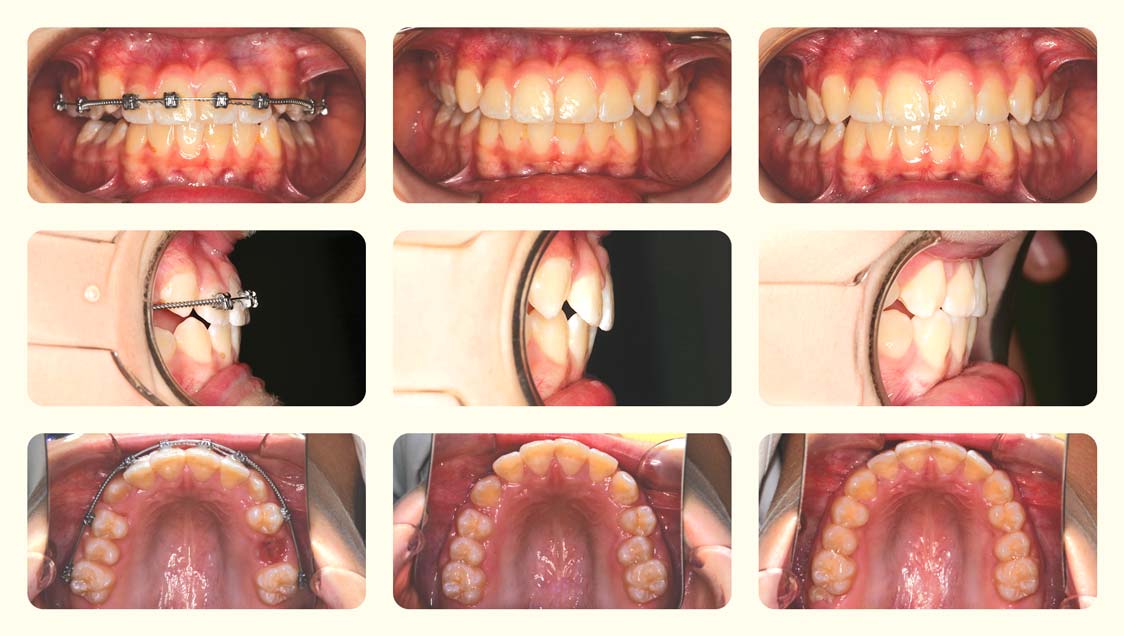
Left column: Six months into treatment.; Middle column: At 10 months.; Right column: Completion at 15 months.
Following the canines dropping into place, the braces were removed, and the treatment was finalised using the Myobrace®T2 (Myobrace® for Teens).
The Myobrace®for Braces (B-series) includes three appliances. The B1 can be used prior to fitting braces or at the point of initial fitting and aims to establish correct nasal breathing and tongue posture.
The B1 allows sagittal correction to begin immediately, prevents initial soft tissue irritation by covering the brackets and wires and separates the arches which allows better development through disocclusion.
The B2 is the next appliance which is to be used once levelling and alignment has taken place. The B2 is a firmer appliance which continues on from the B1 benefits and works further to improve the swallowing method by restricting the use of the buccinators and mentalis muscles, allowing only the tongue to function during the swallowing process and allows for better arch development.
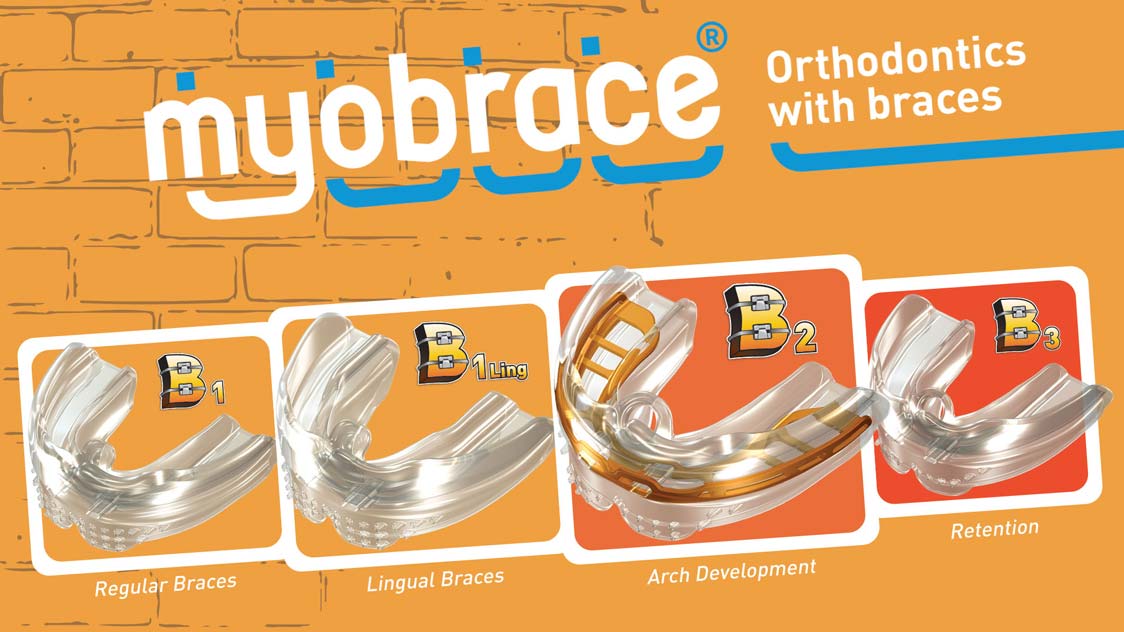
The B3 is the retention appliance to be used once the braces have been removed and the patient is in removable vacuum formed retainers. The B3 works to maintain the sagittal correction which has taken place throughout treatment until neuromuscular adaptation has taken place.
Muscle adaptation is the part of orthodontic treatment which takes the longest to alter, whereas alveolar bone remodels in 3-6 months, condylar remodelling takes around 6-12 months and neuromuscular adaptation can take up to 12-24 months.[16][17]
Thus, a retention appliance which holds the sagittal correction is essential following any orthodontic treatment. Stabilisation and maintenance of therapeutic goals become part of the lifelong learning and change process.[5]
Interested in learning how to use MRC's appliances?
Our FREE foundation course is the perfect starting point for any healthcare practitioner wanting to learn how to use our treatment systems.